 Video
Video Reviews
Reviews Gallery
GalleryPage Contents
- 1. What is Breast Reconstruction?
- 2. What Are the Different Types of Breast Reconstruction?
- 3. When is Breast Reconstruction Done?
- 4. What to Expect From Breast Reconstruction
- 5. Breast Reconstruction with the Goldilocks Technique
- 6. Who is a Candidate for Breast Reconstruction?
- 7. Which Breast Reconstruction is Best?
- 8. How Long Does Breast Reconstruction Last?
- 9. Breast Reconstruction Recovery
- 10. Breast Reconstruction Complications
- 11. Schedule a Consultation
- 12. Breast Reconstruction FAQs
What is Breast Reconstruction?
Breast reconstruction is an important plastic and reconstructive surgery that can give patients back the breasts they once had, lessen the physical and mental impact of a mastectomy, and help ensure patients maintain their self-image. Breast reconstruction is done after a mastectomy (delayed reconstruction) or on the same day (immediate reconstruction), and there are a few different reconstruction options, including implant-based, Goldilocks, and flap reconstruction.
Implant breast reconstruction surgery uses saline or silicone gel breast implants to form a new breast mound, while flap reconstruction (often called autologous tissue reconstruction) takes tissue from another part of your body to form a new breast.
The main goal of breast reconstruction is to restore one or both breasts to near-normal shape and improve issues with symmetry, appearance, and size following a mastectomy or lumpectomy. It can be done immediately after your mastectomy or at a later date. Reconstruction may be one surgery or multiple surgeries.
What Are the Different Types of Breast Reconstruction?
There are two types of breast reconstruction, autologous tissue reconstruction and the implant reconstruction. Autologous tissue reconstruction is using your own body tissue from another location to make a new breast. In plant reconstruction is using a silicone implant, similar to what’s used in breast augmentation to reconstruct a new breast. Some of the advantages of autologous tissue breast reconstruction include a breast that is softer and feels more natural, since this is your own tissue once the wounds are healed this tissue will be there for life and not require additional surgery and if the abdomen is used as a donor source you also get a tummy tuck. Implant reconstruction has advantage of a faster recovery and there is no donor site morbidity. The disadvantage may be an implant is a machine and could leak in a lifetime and require additional surgery.
 Real Patient
Real Patient
Reviews
I had a great experience with Dr. Perry and his staff! He really wanted to see my progression all the way through, and still checks in.
MoreWhen is Breast Reconstruction Done?
The breast reconstruction can be done as an immediate reconstruction or a delayed reconstruction. The advantage to immediate reconstruction is that the skin envelope left after the mastectomy can be used to generate a more natural-looking breast and the patient wakes up from the mastectomy surgery with the breast mound as opposed to a flat chest. The advantage of a delayed reconstruction is that if additional procedures like radiation or chemotherapy are needed these procedures will not damage the newly reconstructed breasts.
What to Expect From Breast Reconstruction
What to expect during your breast reconstruction depends on the type being done. There are a variety of different types of breast reconstruction.
With implant reconstruction, breast implants are used to form a new breast mound, while flap reconstruction takes tissue from another part of your body (usually the lower belly) to form a new breast. There are also a variety of types of flap reconstruction. Dr. Perry will discuss your options with you during your consultation.
No matter the type of breast reconstruction you have, we will administer general anesthesia to ensure you’re completely comfortable throughout the procedure. Incisions will be made along the breasts to either insert implants or place new tissue. When the breasts have been reshaped, Dr. Perry will then close the incisions, and you’ll be ready to start your recovery.
Breast Reconstruction with the Goldilocks Technique
Besides the flap and implant-based breast reconstruction, there is also the Goldilocks technique. With this breast reconstruction procedure, the remaining fatty breast tissue and skin that isn’t unhealthy and removed during a mastectomy will be used to form a new breast mound. This means no implants or tissue from other areas of the body will be needed.
The Goldilocks procedure is typically appropriate for patients with larger or heavier breasts, but those with smaller breasts may be good candidates as well.
The Goldilocks technique can also give patients a template to work from for future breast reconstruction procedures.

Featured Procedure Video:
Video Transcript:
When we talk about reconstructive breast augmentation, what I really mean is a secondary augmentation where we’re trying to make corrections on problems that exist. The key to doing a reconstructive type augmentation is the analysis. Trying to figure out what’s wrong is the first step to being able to solve a problem and make a correction. The second thing is to make your plan on what you can do to try to solve the problems and then move from there. This first patient, what we’re looking at is a misplaced implant on the left side. Now this implant is too low on the left side and it’s also just a little bit too low on the right hand, on the right side. The key to augmentation is one, picking the right implant to fit the skin that’s available and making a pocket in the appropriate location. The pocket for breast augmentation should be centered around the nipple, that’s the key. We don’t want to have, you know, too much implant above the nipple, too much below, too much to the right or too much to the left. If our implant is too high it makes the nipple point down, if our implant is too low it makes the nipple point up. If the implant is too far the left, it makes nipple turn to the right. If it’s too far to the right, it makes the nipple turn to the left. So centering the implant behind the nipple is the key. And what we see in the first patient is that this patient on the right side has more implant below the nipple than above, on the left side has much more implant below the nipple than above. There’s only implant to this length here, two times to three times as much below. So what we need to do is reestablish the pocket in this patient in the proper location so the implant will be in the appropriate location.
So you can also see from the pitcher from the angle on the lateral angle, the oblique picture, the implant starts here and ends here. So we have 75% to 80% of the implant below the nipple, so that’s inappropriate. If we look on the right side, here we can see the distance from the top of the implant to the nipple and from the nipple down, we still have more than 50% of the implant below the nipple. So both the implants are low with the left one being extremely low. So what we did was we went into surgery, opened around the areola, removed the implant, and then we adjusted the pocket. We used plication sutures on the inside, used some of the capsule that’s present after breast augmentation to augment and strengthen this lower pocket, and to close off this pocket to put the implant in the appropriate location. And this is an early post up photo, you see still some scarring in place, some scabs in place but we have a more symmetric appearing augmentation with the nipple appearing in the middle of the implant. We can see roughly the same amount of implant above and below the nipple and they have the same thing on both sides. So we readjusted the pockets on both sides to sim the nipple.
Now we can see laterally some of the plication points from inside that we used to reestablish the pocket, securing that pocket down to even ribs and even the fascia of the muscle below to get a secure fixation of that lateral pocket where you can see an even lateral pocket here as opposed to lateral pocket extended into the axilla. Now this is a picture some weeks later after the healing has taken place and we still see the symmetry of the implants. We see again 50% of the implant is above and 50% of the implant below the nipple. And when we look to the side, all the plication sutures have dissolved and we have a nice appearing shape on the lateral board of the implant. So this is what we’re trying to do, trying to restore the implant to its proper location and center the implant behind the nipple. This is an extreme example again, where we can see variable implant above the nipple and all the implant below the nipple.
The second case we have is a case of what we call tubular breast or tubular changes in the breast. And we see a difference between the right and left breast with the right breast being a tubular change. Now what is a tubular change? A tubular change is a high fold, high inframammary fold and the breast tissue herniated behind the nipple and pulled away from the chest wall. If you can see on the right side, most of the breast tissue is here near the nipple. On the left side, most breast tissue is near the chest wall. So that’s our analysis, we have a fold that’s too high and displaced breast tissue. So what do we need to do, and again, you can see it from the lateral to more extreme and more extreme measure, all the breast tissue is here, it is not against the chest wall. On the normal side, there’s more tissue on the chest wall. So what we need to do is move the breast tissue back towards the chest wall, and then we need to work on exploring this inframammary fold. And the augmentation can do this. So what we did was we weakened the tissue from the inside and level the fold to allow us to create a new fold. So our goal here is made a new a new fold at a similar height to the previous fold.
The other thing we did was using the incision on what place the nipple is we actually replaced the breast tissue and pushed it back towards the chest wall and away from the nipple. So we can create a nipple as opposed to the herniated look we see here. So those are the two… those are the problems with the tubular breast and those are the corrections. We use the sutures to create a cone shape of the nipple and to push the breast tissue back towards the chest wall. And then we used weakening inside the tissue after we created the space under the muscle, we weakened the tissue of the previous fold and then created a new fold and we can see a greater symmetry between the breast from before.
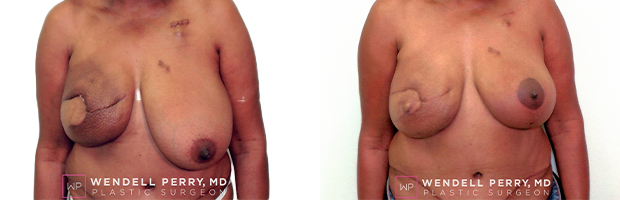
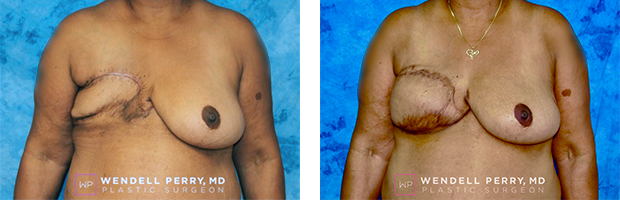
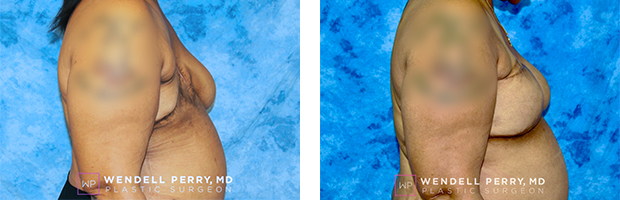
This next patient is a patient who has problems with scar tissue on the bottom of the breast below the nipple and loss of volume in the bottom of the breast below the nipple. That’s our analysis of problem. I think our implants are in relatively good position. So what do we need to do? We needed to create volume, and we needed to try to weaken some of the scar tissue. So we can see the indentations for the loss of volume and indentations from the loss of volume. So what we used, our plan to correct this volume problem was one, we use what’s called a dermal matrix. A dermal matrix is really a skin and it could be human skin, it could be animal skin, or even could be an artificial matrix that is used to create in-growth of your own tissue in order to fill volume. So we used a dermal matrix on the right side along with fat transfer. We harvested fat from other areas and injected the fat into the skin to create volume. Again we needed volume. We use the liposuction cannula to destroy some of the scar tissue to allow the skin to expand. On the left side, which the problem was not as bad as the right, we did not use a dermal matrix and just used 100% of fat injection in order to fill that loss of volume. And you can see we have a very good correction, not complete correction but much better than before. A second round of fat injection could be attempted in order to fill that deficit of tissue here. But we can see that the fat transfer can make a difference in problems like this for breast surgery.
Now we have another patient that had a previous augmentation. And again, we’re dealing with inappropriate location of the implant. The implant is not centered behind the nipple. If you look, you can kind of see the implant’s centered here to here with no implant really below the nipple. You can see the shape and the high point of the implant here instead of the high point of the implant behind the nipple. There is no added volume really from the nipple down and that’s why we have this appearance. So the point of making this correction is to center the implant behind the nipple. So we went in through the areola, and removed the old implant, adjusted our pocket because the pocket really determines where the implant sits, and we corrected the pocket to leave the pocket around in its proper location. And now we have an implant that’s centered behind the nipple, where you can see more projection at the nipple with a normal natural shape of the breast tissue. So this is a problem of the implant location and the implant again not being centered behind the nipple.
Here’s another example of the inappropriate location of the implant. When we do breast augmentation, a lot of times patients want cleavage, want the breasts to be close together. That’s a good thing to want but we must still follow the rules of keeping the implant centered behind the nipple. If we put all the implant inside of the nipple, the nipples will point out and we won’t have a natural appearance. So this is what happened in this case, the implants again start here and finish here. Now we have 70% to 80% of the implant on inside the nipple, and only 20% of the implant outside the nipple. So that’s the problem with this, this patient to want to go very large, so we accommodated with large implants. But if you see again, now the nipples instead of pointing to the side are pointing more straight ahead, and now we have more symmetric with implant to the left of the nipple, implant to the right, implant the left and right. So that is kind of the key to the breast augmentation is centering the implant behind the nipple. It’s always a mistake to move the implant above below to the left or the right of the implant. You have to center the implant. The distance of the implants being apart is really determined by the nipple and the size of the implant you use, not how you sit the implant in the pocket. If you don’t make the pocket correctly, you don’t have a good appearance.
Now this case is showing capsular contracture. This patient had capsular contracture on the left side with a rupture and now we’ve seen the implant is raised. Again, the implants again are too high. The implant is starting here and then ending here, the implant is not centered. Again, you can see the peak of the implant here so the implant is in the wrong location. So what was done for the end, the other problem we have is the nipples are at different heights. This person had to lift on the pass and the nipples are at different heights. So what we’re trying to do is get a more symmetry and to remove the capsular contracture and center the implant. So those are after. If you can see what we’ve done, we’ve got the implant more centered and have more natural appearance behind the breast. We’ve removed the capsular contraction removed the scar tissue and now we’ve also moved the nipple up on the left side. So we have more of a symmetry with more of the nipple centered behind the… with the implant centered behind the nipple, the nipples are more symmetric appearance.
This is another example of the implant being used to try to create cleavage where the implant was put too close to the midline. Again, with the nipple here, we have, you know, over 80% of the implant inside the nipple and only 20% outside so the nipples point out and also the nipple is too high, the implants too high, so nipples point down. So what we did was we repositioned the implants, readjust the pocket, now we have more of a naturally appearing augmentation with the implant below to the side and inside of the implant.
Again, we have a another example of the implant being high. Again you can see the peak of the implant here, the implant is too high, and we don’t have the same amount of implant below the nipple, so we reposition the implant with a larger implant and now we have the implant below the nipple, above the nipple, and into the sides. Again, the trick is to center the implant. So these examples are showing things that you can do to try to make corrections with implants. I think what the things we can take out of this is that the implant needs to be centered behind the nipple. That’s the key fact in doing a breast augmentation. The other thing we can see is that fat can be used to fill deficits and make corrections with implants along with the use of dermal matrix. So these are some examples of correction you can make with breast augmentation. Thanks for watching this video and we’ll try to create more videos and make an educational video library. Take care.
Who is a Candidate for Breast Reconstruction?
Ideal candidates for breast reconstruction include patients who meet the following criteria:
- Have realistic expectations
- Have a positive outlook
- Nonsmokers
- Don’t have any additional medical conditions that could negatively affect the surgical or recovery process
- Want to regain their breast shape
- Want to feel better about your body
- Have undergone or will undergo a mastectomy or lumpectomy
Which Breast Reconstruction is Best?
Which breast reconstruction technique is best for you depends on a number of factors, including the type of mastectomy you had, your body type, your breast cancer treatment (if radiation therapy is done, you may need to wait until after treatment), and your preferences and goals.
Implant reconstruction often comes with a faster recovery process as there is no donor site where tissue is being taken from, but implants can leak and require additional surgery. Flap reconstruction allows for softer, more natural results, and additional surgery is often unnecessary once results have been achieved.
As for the Goldilocks technique, you don’t have a second donor area that needs to heal, so recovery can be quicker than with flap reconstruction, but the resulting breasts tend to be smaller and have less volume when compared to implant reconstruction. Although, it can depend on how much existing tissue and skin are available to create the new breast mound.
How Long Does Breast Reconstruction Last?
How long your breast reconstruction lasts depends on the reconstruction technique used. With breast implants, you typically need to replace your implants after 10-15 years. With a flap reconstruction, the results are considered permanent, but changes in weight and the natural aging process may affect the look of your breasts.
For the Goldilocks technique, results are considered permanent but can be affected by weight changes, gravity, and the natural aging process.
Breast Reconstruction Recovery
Depending on the reconstruction technique used, recovery can take 6-8 weeks, with full results taking several months. Implant-based reconstruction has a shorter recovery period than flap and goldilocks reconstruction. Flap reconstruction also involves the healing of the donor site to consider.
You will likely need to take 2-4 weeks off work if you have a desk job, while those with more physically demanding jobs will need 6-8 weeks off work. You’ll need to limit your movements, but light, gentle movements are encouraged soon after surgery.
Breast Reconstruction Complications
The complications associated with a breast reconstruction could be a loss of the reconstruction, wound healing problems, hernia, hematoma, infection, capsular contraction, implant failure and the complications of anesthesia.
Schedule a Consultation
Have you had a mastectomy and are looking to have your feminine curves back? Or perhaps your mastectomy is coming up, and you want to have immediate reconstruction on the same day? We’ll meet all your needs at Wendell Perry, MD! Take the first step and schedule a consultation today. Call our Miami, FL office or message us using our online contact form.
 GALLERY
GALLERY LOCATIONS
LOCATIONS